COVID-19 was the crisis of a generation. Our front liners, including nurses, doctors, cleaners and drivers, responded heroically in the face of an enemy that we knew little about before 2020. Words cannot repay the debt of gratitude we owe each one of them.
COVID-19 also took the lives of over 1,700 people in Singapore. I extend my deepest condolences to their families for their immeasurable loss.
While I acknowledge that the Government has performed well in many aspects of its response to this pandemic, it is important that we do not get carried away patting ourselves on the back to the exclusion of implementing the important lessons learned during this crisis. We need to better prepare ourselves for future pandemics, which are likely to be more frequent and severe, not least because of increasing globalisation and urbanisation.
Healthcare capacity
Healthcare capacity was stretched even before COVID-19 hit. The pandemic exacerbated this capacity crunch. Many healthcare workers reported working long hours overtime, being recalled for duty on their days off and even having no time for toilet breaks. The White Paper highlighted challenges in staffing hospitals with healthcare workers, resulting in existing workers feeling fatigued and burnt-out from the prolonged crisis.
We are now no longer fighting COVID-19 like before, yet the shortage of healthcare facilities and manpower still persists. For example, median waiting times for emergency cases that require hospital admission from January to September last year was about seven hours. This can spike to 50 hours during infection waves.
In October 2016, then-Minister for Health Gan Kim Yong launched the Healthcare Manpower Plan 2020, which highlighted the need for 30,000 more healthcare workers from 2015 to 2020 to look after Singapore’s fast-ageing population. It is now 2023. How many of these 30,000 additional healthcare positions have been filled? During the debate on the Healther SG motion last October, Minister Ong Ye Kung said that another 24,000 nurses, allied health professionals and support care staff are needed to operate hospitals, clinics and eldercare centres by 2030.
Recruitment alone is not sufficient. There needs to be a corresponding transformation in the remuneration of healthcare workers. The group that bore the heaviest burden of caring for COVID-19 patients were nurses. Their long working hours and lower starting pay compared to territories like Australia, Hong Kong and Canada, could have contributed to their high attrition in recent years. In 2021, the proportion of nurses resigning hit a five-year high, with 7.4% of local nurses and 14.8% of foreign nurses leaving their jobs.
Why are so many nurses leaving the healthcare sector? A study on healthcare workers conducted by researchers Celene Ting and others from the Saw Swee Hock School for Public Health, Tan Tock Seng Hospital and the NCID highlighted that healthcare workers reported burn-out from being overworked, emotional exhaustion and at times feeling a lack of appreciation or support at work.
This was exacerbated by having to care for difficult and sometimes abusive patients. Nearly a third of healthcare workers witness or experience abuse each week, according to a tripartite workgroup’s findings, which SPS (Health) Rahayu Mazam shared earlier this month during the Committee of Supply debate.
Additionally, some healthcare workers are also drawn to work opportunities overseas, where they can receive higher remuneration and more societal recognition. For example, a nurse that CNA interviewed mentioned that after moving from Singapore to the United States, he felt more highly esteemed by the public, citing an example of how his car loan was approved immediately after he said he was a nurse, despite having no credit history.
Urgent changes are needed if we are to reverse the departure of nurses and boost their numbers in Singapore.
Nurses’ basic pay should be benchmarked to that of their contemporaries in other essential public services, a point made by Associate Professor Jeremy Lim from the Saw Swee Hock School of Public Health during a recent CNA interview. Such services could include the police, army and the education service. The salaries of nurses in other jurisdictions like Australia, Hong Kong and Canada should also be considered in the benchmarking.
It should take into account the longer hours that nurses have to work compared to many other professions. This is to ensure that the opportunity cost of taking up nursing instead of another profession would be minimised. We also need to make the nursing profession more highly esteemed by the general public.
Another way to attract more Singaporeans to take up nursing and increase retention would be to enhance their professional development opportunities. Nurses in Singapore are often still seen as the assistants to doctors instead of being professionals in their own right. They should instead be granted more autonomy and entrusted with higher level responsibilities. In the United Kingdom, nurses run clinics, diagnose patients, take on high-level management roles and help to lead medical research. We should accelerate efforts to achieve the target of 700 Advance Practice Nurses by 2030.
Beyond pay, management culture, work recognition and working hours are also areas that need to be examined for a holistic improvement of the profession.
Including PwDs in pandemic response measures
During the pandemic, many people with disabilities (PwDs) experienced difficulties coping with measures such as the blocking off of regular entrances and exits, shifting access points for PwDs, and having to locate and scan SafeEntry codes. Many wheelchair users and people with developmental disabilities, visual impairments and autism spectrum disorder had difficulties with SafeEntry scanning. Measures such as COVID-19 swabbing and mask-wearing were difficult for some people with mental disabilities. I recall a resident of mine who was very worried that her son, who had a mental disability, would struggle and hurt himself when made to undergo mandatory swabbing at his block when an outbreak occurred there.
While support for PwDs was eventually introduced, much of this was reactive. This could be due to an absence of meaningful participation by PwDs when safe management measures were implemented.
Moving forward, it would be advisable to have at least one member of the disability community on emergency task forces so that the community’s views can be adequately represented. More importantly, all policies rolled out need to take into account the unique needs of PwDs, to ensure that they are not excluded.
Honest communication with Singaporeans
The next section of my speech deals with the public communication on pandemic mitigation measures.
In January 2020, the Government issued an infographic titled “Advisory on wearing masks” which highlighted that “masks are generally not needed for people who are well.”
The infographic, which was also posted on social media, added that “there are sufficient masks in the warehouses and government stockpiles.”

The then-chairman of the PAP’s Government Parliamentary Committee for Health, Dr Chia Shi-Lu, echoed the Government’s line later that month when he told the New Paper that “surgical masks can prevent the passing of virus from a wearer, but when it comes to protecting (a healthy wearer), the masks won’t protect from viruses.”
The Prime Minister, in January 2020, said Singaporeans should follow doctors’ advice on how best to protect themselves from the virus, which includes not wearing a mask unless they are unwell.
The PM rightly pointed out though, that the “Wuhan virus” — as it was then called — was “probably more infectious than SARS, and possibly infectious even before people have symptoms.” This was on 31 January 2020.
The fact that the Government knew in those early days that asymptomatic transmission of the virus could occur should have prompted them to advise everyone to wear masks when in contact with other people.
On 10 February 2020, four local doctors did just that by issuing a statement urging Singaporeans to wear masks always when leaving home, even if they were well. Dr Colleen Thomas, Dr Judy Chen, Dr Tham Hoe Meng and Dr Lim Pin Pin acknowledged the difficulties in obtaining new surgical masks every day, and urged the use of creative solutions like washable cloth masks or scarves. They pointed out that these measures were better than no mask at all.
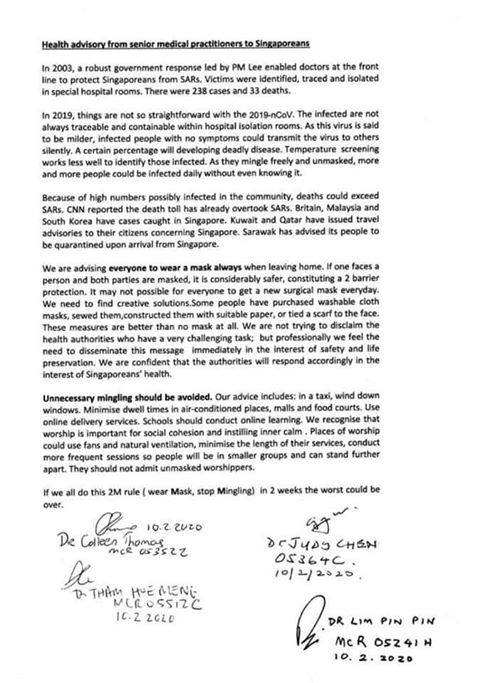{kind=link}
In response to the four doctors a few days later, the Director of Medical Services at MOH said that “it is not wearing masks that’s most important, it’s hand washing” — even though the two actions were not a binary choice. The Straits Times ran an article to “educate” the public on questions like, “Is it really true that you do not need to wear a mask if you are not sick? Is hand washing better protection against viruses than a mask?”
These statements were incongruous and did not seem to be consistent with common sense. People intuitively knew that any layer preventing the spread of droplets would be better than not having one.
It took a leaked recording of a Minister at a closed-door meeting in February 2020 to reveal that Singapore was rationing masks to save them for healthcare workers.
The White Paper stated that “in hindsight…the government could have encouraged Singaporeans to devise their own face masks while we set up manufacturing lines to ramp up production of surgical masks.” This was not hindsight — it was what the four doctors advised in the first place, which the Government did not heed.
It took another three months for the Government to stop discouraging people from wearing masks by “updating the guidance” on 3 April 2020. The result of the about turn, as acknowledged in the White Paper, was that public trust in the Government was eroded. Singaporeans saw through the Government’s initial statements about the real reason why they were discouraging those who were well from wearing masks — it was because there were insufficient supplies of surgical masks, not because mask wearing was less effective than hand-washing.
While concerns over panic buying and hoarding by the public were not unfounded, the Government had stockpiles of surgical masks for healthcare workers and should have had the power to requisition more masks from the commercial market.
This brings me to my next point: Why did Singapore not have sufficient domestic capacity to manufacture items as basic as face masks? Was the Government not able to marshal local companies to accept and prioritise contracts for the manufacture of materials deemed essential for our defence against COVID-19, including face masks and ventilators?
Domestic manufacturing capacity during crises
The White Paper mentioned that the COVID-19 (Temporary Measures) Act gave the government the option of mobilising civilian resources using the Requisition of Resources Act (RORA), but chose not to use those powers. Instead, the government said it will leverage alternative structures — for example, through strategic partnerships or cooperation agreements — to effectively harness civilian resources for crises. I agree that it would not have been appropriate to use RORA for the COVID-19 pandemic, given that the Act is a rather blunt tool which is meant more for wartime scenarios than a public health crisis.
In any case, RORA does not appear to give the government the authority to ask the private sector to prioritise orders from the government, short of requisitioning the entire line of services. For example, it is not clear if the government can ask a company to prioritise orders from the government for the manufacturing of masks, without requisitioning and running the entire mask production facility on its own.
Will the Government consider legislation akin to the US Defense Production Act, which empowers the executive to direct private companies to prioritise orders from the federal government and take actions to restrict the hoarding of needed supplies?
The role of Temasek
I now turn to the role during the pandemic played by one major local company — Temasek Holdings.
Temasek-linked companies played an outsize role during the pandemic. Almost all the private sector partners named in the White Paper are Temasek-linked companies. The White Paper stated that private sector partners like Temasek were “indispensable” sources of support during COVID-19. This may point to an over-dependence on the Temasek ecosystem. Would it be better to diversify the base of private sector partners that can support the national effort in times of crisis?
During Question Time on March 3rd, I asked SMS (Finance) Chee Hong Tat if the Government’s total COVID-19 spending of $72.3 billion included the amount spent by Temasek Holdings, Temasek Foundation and other Temasek-linked companies for their COVID-19 activities. The SMS gave a rather convoluted answer but I believe the answer was “No”.
This being the case, can I ask: How much did Temasek and its related organisations spend out of their own budgets on COVID-19 initiatives like face masks, hand sanitiser and oxygen concentrators which were made available locally and overseas?
The White Paper stated that “While Temasek’s main goal remains to deliver long-term returns on its assets, it plays a unique role in supporting a robust portfolio of local companies that can anchor important capabilities for Singapore in a crisis.”
Does Temasek have goals other than to deliver long-term returns on its assets? Is this “unique role” part of the Government’s mandate for this Fifth Schedule company?
I appreciate the work that Temasek companies and their employees did to keep Singaporeans safe during the pandemic, and the resources they spent doing so. But I think it is important for the House to know if Temasek’s expenditure on COVID-19 constitutes a draw on our reserves and, if so, whether the approval of the President was sought and obtained?
Conclusion
Sir, it is a truism that those who do not learn history are doomed to repeat it. Notwithstanding the absence of a Committee of Inquiry, which the Workers’ Party had called for, we still have many lessons to learn from in the White Paper and this debate.
For the sake of our future generations who may have to go through catastrophic pandemics like these, we have to both learn and implement these lessons.
In this spirit, Sir, I support the motion.